

Most people know that menopause brings hormonal shifts, hot flashes, and changes in mood and sleep. What tends to get less attention is what those same hormonal changes do to your teeth and gums. The mouth is more sensitive to fluctuating estrogen levels than most people realize, and for women going through perimenopause or menopause, that sensitivity can translate into real dental problems, including a higher risk of tooth infection.
This blog looks at the biological connection between menopause and oral health, what specific risks emerge during this stage of life, and what you can do to protect your teeth, starting with routine care and knowing when something needs more than a cleaning.
The Hormonal Connection to Dental Health
Estrogen plays a more significant role in oral health than most people are taught. It supports blood flow to gum tissue, helps maintain the bone density in your jaw, and contributes to saliva production. When estrogen levels drop during menopause, all three of those functions are affected, and each one has a downstream effect on your risk of developing tooth decay, gum disease, and pulp infections.
Patients who come to Irvine Smiles Dental for root canal treatment in Irvine often
don’t realize that their recent spike in dental problems correlates with hormonal changes they’re experiencing. Putting those two things together earlier would have allowed for preventive steps before infection reached the pulp.
How Menopause Creates Conditions for Tooth Infection
The connection isn’t direct in the sense that menopause causes root canal infections on its own. Rather, it creates several oral health conditions that, left unmanaged, raise the probability of reaching that stage.
Dry Mouth and Reduced Saliva Flow
Saliva does more work in your mouth than most people give it credit for. It neutralizes the acids produced by oral bacteria, rinses away food debris, and delivers minerals that help remineralize enamel. During menopause, lower estrogen levels can reduce saliva production, a condition called xerostomia. A drier oral environment allows bacteria to thrive, accelerates enamel erosion, and increases the rate of decay. Untreated decay that reaches the dental pulp becomes a root canal situation.
Gum Tissue Changes and Periodontal Risk
Estrogen helps maintain healthy gum tissue, and its decline during menopause can lead to gum thinning, increased inflammation, and greater susceptibility to periodontal disease. Research published in the journal Menopause has found a significant association between postmenopausal status and periodontal disease, particularly in women not on hormone replacement therapy. Periodontitis doesn’t just affect gums. As it advances, it can expose root surfaces to bacteria and create pathways for infection to reach the inner tooth.
Bone Density Loss in the Jaw
Osteoporosis, which disproportionately affects postmenopausal women, has well-documented effects on jawbone density. Lower alveolar bone density reduces the structural support around teeth, increasing mobility and making teeth more vulnerable to trauma and infection. A study published by PubMed shows that postmenopausal women with osteoporosis had significantly higher rates of tooth loss and periodontal bone loss than those without. When the bone surrounding a tooth’s root weakens, bacterial infection has less resistance to work against.
Burning Mouth Syndrome and Altered Sensation
Burning mouth syndrome, characterized by a persistent burning or tingling sensation in the mouth, tongue, or gums, occurs more frequently in perimenopausal and postmenopausal women. While it isn’t directly linked to infection risk, it can make it harder to identify genuine pain signals from a tooth with developing pulpitis. When discomfort becomes a constant background, early warnings from a problematic tooth can be missed.
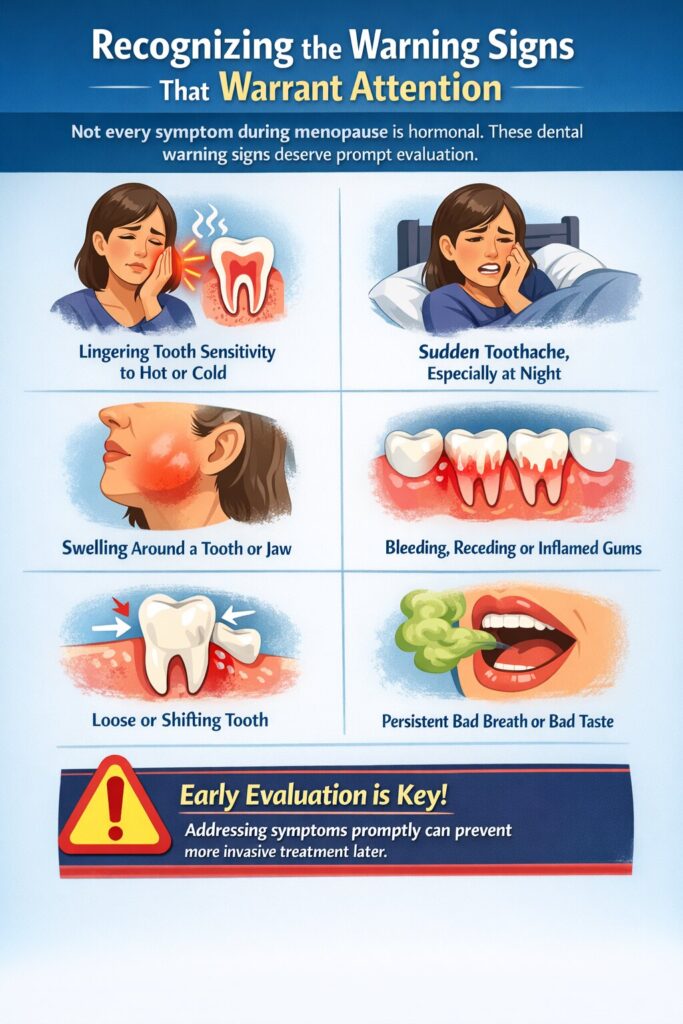
Recognizing the Warning Signs That Warrant Attention
Not every symptom during menopause is hormonal. Some dental warning signs deserve prompt evaluation regardless of what else is happening in your body. These include:
- Tooth sensitivity that lingers after exposure to hot or cold, rather than fading within a few seconds
- Spontaneous toothache, particularly pain that wakes you at night or occurs without any obvious trigger
- Swelling around a tooth or in the jaw
- Gum tissue that bleeds easily, recedes, or appears unusually red or tender
- A tooth that feels loose or has visibly shifted position
- Persistent bad breath or a bad taste in the mouth that doesn’t improve with brushing
These symptoms don’t automatically mean you need a root canal, but they all deserve professional evaluation sooner rather than later. What starts as reversible pulpitis can become irreversible quickly, and the window for the least invasive treatment closes fast.
How to Protect Your Teeth During and After Menopause
The increased risk is real, but it’s also manageable. A few targeted adjustments to your dental routine can significantly lower your chances of developing an infection that progresses to the point of needing endodontic treatment.
- Stay hydrated: Water helps compensate for reduced saliva flow. Sipping water throughout the day, especially after meals, keeps the oral environment less hospitable to decay-causing bacteria.
- Ask about fluoride: Prescription-strength fluoride toothpaste or in-office fluoride applications can reinforce enamel that’s under increased acid attack due to dry mouth.
- Keep up with periodontal care: If your dentist has noted gum recession or bone loss, moving to three or four cleanings per year instead of two is a proactive and evidence-backed approach.
- Tell your dentist about medications: Several medications prescribed for menopause symptoms, including antidepressants and antihistamines, contribute to dry mouth. Your dentist should know what you’re taking.
- Don’t delay treatment: A small cavity caught during a routine dental exam can be fixed with a filling. That same cavity, ignored for another year, can become a root canal. During menopause, the timeline from minor decay to pulp issues can be shorter than it would have been earlier in life.
Your Smile Deserves the Same Attention as the Rest of Your Health
Menopause is a significant hormonal transition, and your teeth feel it even if no one has told you to expect that. If you’re noticing changes in your gum health, increased sensitivity, or dental discomfort that feels different from what you’re used to, those signals are worth taking seriously.
Book an appointment at Irvine Smiles Dental. Our team will assess your current oral health in the context of your whole health picture and help you stay ahead of the issues that menopause can quietly set in motion.
People Also Ask
Does hormone replacement therapy protect against dental problems during menopause?
Some research suggests that hormone replacement therapy (HRT) may help preserve jawbone density and reduce the severity of gum tissue changes associated with estrogen loss. A study in the Journal of the American Dental Association found that postmenopausal women on HRT had lower rates of tooth loss than those not on therapy. However, HRT is not prescribed for dental purposes, and the decision involves broader health considerations. Talk to your physician about whether it’s appropriate for your overall menopause management.
Can dry mouth during menopause cause permanent tooth damage?
Yes, if it goes unmanaged. Chronic dry mouth accelerates enamel erosion, raises decay rates, and can cause gum irritation over time. Fortunately, it’s also one of the more manageable menopause-related oral health issues. Staying hydrated, using alcohol-free mouth rinses, and speaking with your dentist about prescription fluoride products can significantly reduce the damage.
Is root canal treatment safe for postmenopausal women on bisphosphonates?
Bisphosphonates, commonly prescribed for osteoporosis, are associated with a rare but serious condition called medication-related osteonecrosis of the jaw (MRONJ). While root canal therapy is generally considered safer than extraction for patients on bisphosphonates, your dentist and prescribing physician should be informed and involved in any treatment planning. This is especially important if you’ve been on intravenous bisphosphonates or have been on oral bisphosphonates for several years.
Why do my teeth feel more sensitive after menopause?
Increased sensitivity after menopause often stems from a combination of gum recession, enamel thinning from dry mouth, and sometimes burning mouth syndrome. Receding gums expose the root surface of the tooth, which lacks the protective enamel layer and responds readily to temperature and pressure changes. If sensitivity is new, worsening, or affecting specific teeth rather than generally, it’s worth getting those teeth evaluated for early decay or pulp involvement.
Should I mention menopause to my dentist?
Absolutely. Your menopausal status, the medications you’re taking, and any symptoms you’ve noticed in your mouth are all clinically relevant to your dental care. Dentists use that information to interpret what they’re seeing, adjust their recommendations, and plan monitoring at the right frequency for your current risk level.

